This A3 Insights is published under our ‘Youth Perspectives’ series, where Population Council colleagues, fellows, interns, and partners under the age of 30 write a data-driven thought piece focused on their own interests and research areas.
This piece, authored by Cara Frances, former GIRL Center staff who led the creation of the A3 Policy Checklist and current PhD student at Drexel University, explores the health and wellbeing of a critically under-researched population, sexual and gender minority adolescents living in low- and lower- middle- income countries.
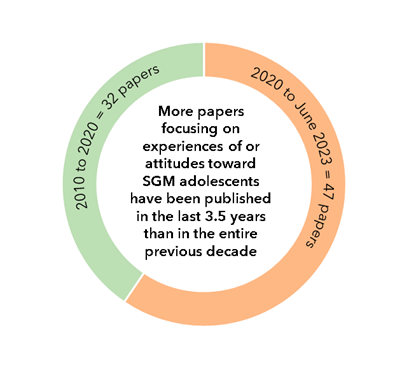
Findings from a recent GIRL Center scoping review demonstrate a much needed, growing interest in the health and wellbeing of sexual and gender minority (SGM) adolescents in low- and lower-middle- income countries. More papers focusing on experiences of or attitudes toward SGM adolescents have been published in the last three and half years than in the entire previous decade (2010-2020: 32 papers, 2020-June 2023: 47 papers). This scoping review, authored by me, Jessica DeMulder, and Camille Garnsey, examined research not only where SGM young people ages 10-24 were centered as the priority population, but also research that explored attitudes of cisgender and/or heterosexual people towards SGM populations.
This research area is growing so fast that over the course of this three-year project, the results changed substantially. When we first shared preliminary results in 2021, the majority of papers that had been published did not include SGM young people as participants. Instead, the papers focused on the beliefs and perceptions of students toward SGM populations or the attitudes of healthcare professionals toward SGM youth.
But this summer (June of 2023) when we checked for new publications, we were excited to see an increase in the number of studies that highlighted the lived experiences of SGM young people. Now nearly two thirds of the papers in our review (50 out of 79) included SGM individuals as study participants. Research that centers on the experiences of SGM young people in low- and lower-middle- income countries is crucial to furthering our understanding of their health, wellbeing, and safety needs and ultimately co-developing interventions to address them.
Looking Ahead Recent data from the United States suggests nearly 20% of Gen Z young adults identify as SGM, making today’s generation of young people not only the largest it’s ever been, but also the queerest. And while the proportion of individuals who identify as SGM varies around the globe, until we have more accurate and disaggregated demographic data on SGM young people globally, we will not be able to fully assess, let alone address, their health and safety needs. The key to increasing research with SGM young people is the leadership and scholarship of SGM researchers. By involving SGM young people in participatory action research as teens or young adults, we can inspire a new generation of SGM researchers and begin to address the inequities that have long prevailed in the global health field. With thoughtful, intentional design, we can build inclusive research teams that promote the leadership of SGM young people, and ultimately their health and wellbeing too.
This A3 Insights describes key elements of the Population Council’s work on the Sahel Women’s Empowerment and Demographic Dividend initiative (SWEDD), which aims to reduce risks and promote opportunities for adolescent girls and young women. The work described in the blog post is executed through UNFPA, the organization tasked with overseeing SWEDD activities and providing technical assistance to SWEDD countries in collaboration with its technical assistance partners (including Population Council). Subsequent posts will cover lessons learned, insights generated, and other related themes from the Council’s SWEDD project. This piece was authored by Miriam Temin (Project Co-Director) primarily, and Anne-Caroline Midy (Project Coordinator).
Unique challenges facing adolescent girls and young women in the Sahel region
During the dynamic life phase of adolescence, many girls in West Africa’s Sahel region grapple with multiple threats to their health and well-being, undermining their potential to access their rights and thrive as adults. Many of these challenges are complex and multi-factorial, reflecting intersecting, long-standing forces and systemic issues. Indeed, the region includes countries with some of the highest rates of poverty, food insecurity, conflict, and population displacement in the world.
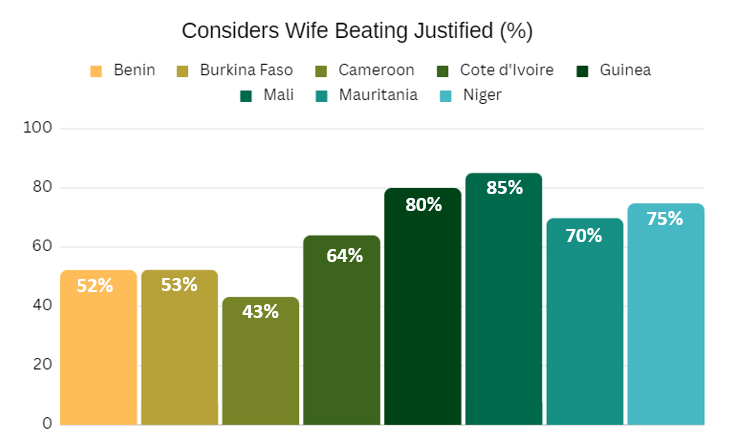
The adolescent indicators dashboard from the GIRL Center’s Adolescent Atlas for Action (A3) provides data for a closer look at various threats in Sahel countries. Using data from nationally representative surveys in Benin, Burkina Faso, Cameroun, Côte d’Ivoire, Guinea, Mali, Mauritania, and Niger, the adolescent indicators dashboard makes a strong case for urgent action for girls and young women in the Sahel.
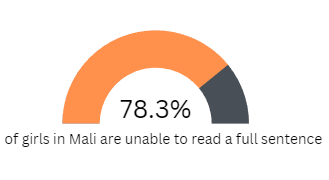
For example, the dashboard shows that in Mali, Guinea, and Cote d’Ivoire, over 20% of adolescent girls have given birth at least once, while in Niger, Mali, and Burkina Faso, that statistic exceeds 30%. 61% of adolescent girls were married or living in union in Niger. In Mali and Guinea, over 60% of adolescent girls consider wife beating justified. Strikingly, the dashboard also highlights that Niger, Guinea, and Mali are among the countries with the highest prevalence of illiteracy in the world, with the vast majority of adolescent girls being unable to read a whole sentence.
Supporting the use of evidence and resources by government and implementing partners
While the Sahel historically has been underserved by overseas development assistance, the current moment provides exciting opportunities as more bi- and multilateral organizations make the Sahel region (and more specifically, French West Africa [FWA]) a priority. Large investments offer the possibility of supporting governments and civil society, growing capacity, and strengthening the evidence base to reduce risks and enhance opportunities for girls.
Funded by the World Bank to the tune of over US$700 million[1] for the period 2014-24, SWEDD’s overall aim is to “increase women and adolescent girls’ empowerment and their access to quality reproductive, child and maternal health services in selected areas of the participating countries” by reducing child marriage, early pregnancy, and girls’ school leaving, inter alia.
SWEDD is a regional activity, expanding from an original six to the current set of nine countries (Benin, Burkina Faso, Cameroun, Cote d’Ivoire, Guinea, Mali, Mauritania, Niger, and Tchad).[2] The governments of these countries lead the initiative, with participation from multiple ministries and implementing partners. Taken together, the range of SWEDD activities was established to position these countries to reap a demographic dividend, whereby rapid economic growth is possible under the right conditions when the size of the young, dependent population shrinks relative to the size of the population of working adults.
Within SWEDD, the Council uses evidence and our capacity, relationships, and tools and other program resources to support activities that target adolescent girls and young women. We do so by strengthening national and sub-national capacity to make evidence-informed use of SWEDD resources based on our large body of evidence on what works and what doesn’t work to reach marginalized adolescent girls and reduce their risks. We aim to increase the quality of SWEDD programming through process documentation; training for managers and implementers on key skill sets; implementation science; regional capacity strengthening workshops, and other activities that aim to promote the use of evidence for action.
For instance, we drew upon effective Council programs to create a second-generation curriculum for mentors in SWEDD’s safe spaces, as well as a bespoke safe spaces minimum standards guide. We developed instructional materials to guide implementers on topics such as non-formal literacy training and operating community-based girl groups during the COVID-19 pandemic. Providing focused technical assistance and strengthening capacity to improve monitoring, evaluation, and learning functions is also a priority area that leverages the Council’s expertise and programmatic resources.
Addressing gendered risks through a multi-sectoral and multi-level approach
SWEDD is uniquely designed to take on the social and structural drivers of gendered risks through a package of programming that is multi-sectoral and works at multiple levels. Its interventions address individuals, communities, local government representatives, and policymakers through the health sector, schools, communities, and demographic researchers. This reflects the importance of socio-ecological approaches to sustainably reduce girls’ risks, based on evidence from the Council and elsewhere.
Recognizing that individuals underlie the summary statistics shared above, the bulk of the Council’s inputs and the largest SWEDD components directly engage community members and adolescent girls and young women (AGYW). Through life skills training in mentor-led safe spaces (espaces surs) groups in communities and schools, mentors aim to equip AGYW with knowledge, skills, and assets to empower them and enable them to navigate risk. In an effort to reap the proven benefits of gender-transformative programming, we support partners to create synergies between safe spaces and SWEDD clubs for husbands and future husbands (clubs des maris et des futurs maris).
Looking ahead: Using early SWEDD lessons to sustain and scale country-owned action
As country-level actors implement the second phase of SWEDD and plans for the third phase take shape, Population Council, along with other technical partners, has a continuing role in promoting evidence, good practice, and learning. Given SWEDD’s large size and ongoing expansion, it will be important to build upon the essential enablers of program success to continue to sustain and scale country-owned action. The multi-sectoral and multi-leveled approach offers countries the opportunity to bring evidence-informed practice together in intentionally selected geographies or ‘hot spots’. Governments in participating countries lead the charge, demonstrating their commitment to SWEDD goals through the involvement of multiple ministries and laying a foundation for sustainability. Furthermore, ownership of SWEDD extends to communities and local opinion leaders including through the active participation of religious leaders in many countries, accounting for the strong influence of community norms in influencing the impact of adolescent girl programming.
At this stage, it is equally vital that lessons from the early days of SWEDD are available and informing expansion, leveraging the regional aspect of the initiative. The Council continues to advance this objective by facilitating cross-learning between country-level stakeholders, documenting and disseminating lessons on ‘safe spaces’ implementation, and using implementation science to identify and expand effective practices that will be feasible and sustainable in SWEDD settings.
This A3 Insights is published under our ‘Youth Perspectives’ series, where Population Council colleagues, fellows, interns, and partners under the age of 30 write a data-driven thought piece focused on their own interests and research areas.
This piece, authored by Tara Abularrage, GIRL Center Intern and MPH candidate at Columbia’s Mailman School of Public Health, centers the recent overturning of Roe v. Wade in the global landscape of abortion policies, outlines the implications of this decision on sexual and reproductive health and rights, and maps current abortion policy indicators across 113 LMICs using the A3 policy checklist.
On June 24, 2022, the United States Supreme Court overturned Roe v. Wade, reversing decades of legal precedent. This makes the U.S. one of only four countries to remove protections for legal abortions in over 25 years. This attack on evidence-based policymaking and the rights of birthing people will have a broader impact on reproductive health, rights, and autonomy in the US and globally.
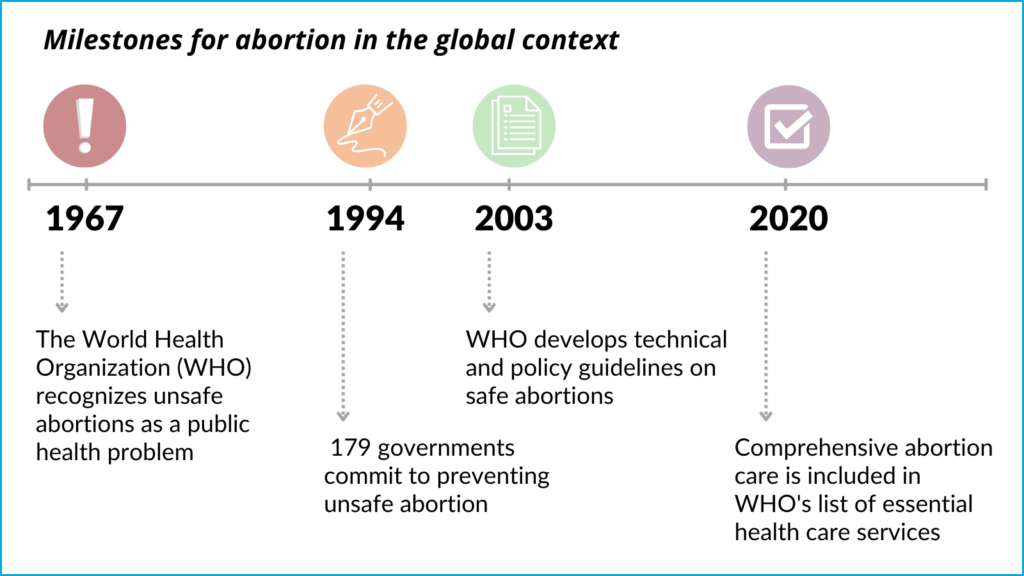
Each year, approximately seventy-three million abortions take place worldwide. Access to safe and legal abortion has been increasingly recognized as a fundamental human right. In 1994, at the International Conference on Population and Development, 179 governments signed a program of action that includes a commitment to prevent unsafe abortion.
The World Health Organization (WHO) recognized unsafe abortions as a public health problem earlier in 1967, and subsequently developed technical and policy guidelines on safe abortions in 2003. As of 2020, comprehensive abortion care is included in the list of essential health care services published by the WHO.
Significant progress has been made in global abortion policy in the last several decades indicating a growing global consensus that access to safe and legal abortion is both a human right and public health imperative. Over the last 25 years, at least 50 countries have liberalized their laws to improve access to abortion care and the majority of countries worldwide do not require parental authorization or notification for adolescents to access abortion services. However, 90 million birthing people of reproductive age still live in countries in which abortion is prohibited altogether. While most countries are taking steps to expand access and grounds for legal abortion, the US stands out with the recent overturning of Roe v. Wade and the enaction of more restrictive abortion policies that have followed.
Need for an enabling environment, especially for marginalized populations
Given the unique set of circumstances and constraints faced by adolescents, enabling laws and policies are even more crucial to support their reproductive health and rights. When accessing abortion services, adolescents face a range of barriers unique to their age group including cost, stigma, lack of confidentiality, misinformation, parental consent or notification laws, and judicial authorization requirements. Such legal requirements prevent adolescents from making autonomous decisions and make it more difficult for them to seek and access abortion care. In Safe Abortion: Technical and Policy Guidance for Health Systems, the WHO recognizes that abortion laws should include protections for informed and voluntary decision-making, autonomy in decision-making, non-discrimination, and confidentiality and privacy for all pregnant people, including adolescents. Additionally, according to this guidance, third-party authorization requirements hinder adolescents’ access to abortion, and increase the likelihood that they will seek unsafe abortions.
The average rate of unsafe abortion is estimated to be more than four times higher in countries with more restrictive abortion laws than in countries with less restrictive laws.
Before Roe was overturned, pregnant people under 18 seeking abortion care in the U.S. already had to navigate a series of legal and logistical hurdles to access appropriate care, and now, post Roe, these barriers have compounded and the process is even more difficult. However, there exists a vast network of activists, providers, and organizers helping pregnant youth access the care they need. While it is currently legal to travel out of state to obtain abortion care in the U.S., there is concern about child custody protection acts, which can criminalize transporting a minor across state lines to have an abortion without parental consent. While the Guttmacher Institute’s interactive map helps track the complex abortion policy landscape for each U.S. state, the Adolescent Atlas for Action (A3)Policy Checklist, created by the Population Council’s GIRL Center, maps national-level policies relevant to the lives of adolescents in 113 low- and middle-income countries (LMICs), including seven key abortion indicators.
What does the global abortion policy landscape look like?
Almost 90% of countries globally allow abortion, at minimum, when the pregnant person’s life is at risk. Abortion is legal to save the life of the pregnant person in 71% of the 113 LMICs included in the A3. While it’s critical to allow abortion in situations where pregnancy poses a risk to a pregnant person’s life, only permitting abortion on this ground is insufficient for guaranteeing birthing people’s human rights.
Only 23% of LMICs (27 countries) have policies allowing legal abortion at the request of the pregnant person, despite the WHO’s guidance that this is the only legal ground which “recognizes the conditions for a woman’s free choice.” These barriers are amplified for adolescents, with only 11% of LMICs (12 countries) that have policies to ensure abortion is legally available to adolescents without parental consent. Such restrictions prevent adolescents from making autonomous decisions and can inhibit them from seeking safe abortion care.
To learn more about the A3 Policy Checklist, review this brief.
Looking ahead
Over the past several decades, incremental and transformative progress in securing legal rights and access to abortion has been made globally. Maintaining this momentum towards liberalizing abortion laws and creating enabling legal and policy environments is critical to ensuring reproductive rights and autonomy, particularly in light of the recent overturning of Roe v. Wade. It’s imperative that countries continue to enact evidence-based policies to support sexual and reproductive health, rights, and autonomy that strive to make abortion available upon request of the pregnant person and make such care universally affordable and accessible. Abortion laws and policies should pay particular attention to adolescents and prioritize their autonomy and access to safe abortion care.
This A3 Insights is published under our ‘Youth Perspectives’ series, where Population Council colleagues, fellows, and interns under the age of 30 write a data-driven thought piece focused on their own research interests. This piece is authored by Yeeva Cheng, GIRL Center Intern, while completing her master’s project designing an online menstrual health education course.
Re-Emergence of Menstrual Cups
A recent GIRL Center-led systematic review and webinar examined menstrual health management (MHM) interventions’ impact on girls’ and women’s education and learning outcomes. While further evidence is needed to determine a causal relationship, there is evidence that interventions targeting both menstruators’i access to MHM materials and reproductive health education improve reproductive health knowledge, increase confidence to manage menstrual health at home and at school, and reduce shame about periods.
In recent years, the menstrual cup has gained momentum as both product and intervention. While earlier prototypes of the menstrual cup were patented as early as the 1870’s, menstrual products requiring insertion, such as tampons and menstrual cups, did not become widely commercialized until the 1950’s, particularly with WWII labor demands shifting menstruators toward public-facing work.
Recent menstrual cup re-emergence and advertising target a specific population of menstruators. In the last decade, cups have been mostly promoted in low- and middle-income countries (LMICs). Like the road to uptake in the United States, lifestyle demands such as increased mobility, have driven cup usage, though not without concerns. A second major driver that affects menstruators in LMICs that did not affect 1950’s American menstruators was the looming threat of climate change.
Menstrual Cups Save—Money and the Environment
Menstrual cups today increasingly advertise being environment-friendly and alleviating “period poverty.” Ranging between 10 to 40 USD with a reusability span of up to 10 years, menstrual cups offer the cost-effective potential to respond to menstruators’ challenges. Since then, over 70 menstrual cup companies have flourished, some with buy-one-give-one plans targeting menstruators in high-income countries (HICs) while distributing or funding a cup in a LMIC context. Such designs are critical in that menstrual cups, while potentially saving between 1700 and 4700 USD of tampons or pads per year, render up-front costs less feasible to menstruators in LMICs. In many cases, menstrual cups are not commonly sold in brick-and-mortar stores and still require online purchasing, creating yet another barrier.
Menstrual cups can save a menstruator between 5,000 and 15,000 pads in a lifetime, an appealing statistic to environmentalists. The plastic in disposable pads can require between 500 and 700 years to dispose, and methods such as crude burning are air-polluting. In the U.S. alone, 9 billion single-useperiod products are consumed each year, with about 80% of these expected to end up in landfills. Even assuming a smaller menstrual product waste footprint in LMIC contexts where disposable materials are used sparingly due to costs, the per capita amount of waste accumulated globally makes the menstrual cup an appealing alternative. Though there have been concerns around menstrual cups and water shortages, a systematic review and meta-analysis on menstrual cup safety, leakage, and acceptability revealed that menstrual cups often result in less use of water when accounting for the water that cloth, cotton, or less structured materials and their leakages might require.
How Educational Policy and Programming Can Reduce Global Period Waste
Menstrual cups minimize both climate and economic costs long-term, but product uptake also requires an enabling environment aided by policy. In building the Adolescent Atlas for Action (A3)Policy Checklist, we checked for the presence of 56 adolescent-relevant national policies in 113 LMICs. These include policies that 1) support MHM education nationally and 2) support MHM education in schools.
Of the 113 countries in the A3 tracker, 22 had MHM policies, and 23 had policy commitments specifically to support MHM in schools. In 10 of these countries, we can observe situations where there are national commitments but not at the school-level, or school-level commitments but no national policies.
Since 2013, UNICEF’s WASH division has focused on countries primarily in South Asia and Sub-Saharan Africa, varying interventions from translating and sharing MHM guides to distributing reusable sanitary pads. However, much of the motivation for promoting reusable and/or natural materials comes down to cost and lack of locally sourced production of materials. While promoting or teaching homemade pad production has been widely popular in LMICs, it is worth noting that these are the contexts that have already been using ecologically safer methods for MHM.
Moreover, LMICs have led innovative approaches to MHM products, curriculum, and integrative policies. Kenya has dedicated research on access to menstrual products in rural and urban areas, contributing to policy written into the Kenyan Constitution’s guarantees toward basic education. Specifically, the Basic Education Amendment Act No. 17 (2017) stipulates a commitment to providing free sanitary towels to all girls enrolled in public education, as well as safe and sustainable means of disposal. Policy Objective 4 lists eight actions outlining how investment, research, and partnerships will collaborate to prioritize recycling, treatment, and waste management. Nepal released a scoping review and preliminary mapping of MHM in 2017, noting commitment to the provision of sanitary pads and disposal facilities. Some policymakers have pointed out that current disposal methods of such products (providing pits and dustbins) are environmentally harmful. Recognizing that it is unfeasible to completely shift away from disposable pads, pragmatic program actions have included installation of disposable pad incinerators in schools to burn pads in an ecologically safe way. While the Philippines has yet to develop a national MHM policy, smaller-scale initiatives have contributed to sustainability efforts. For example, EmpowHer has re-adapted the disposable pad using locally sourced, biodegradable products (corn cob, rice paper, and water hyacinth) that include destigmatizing messaging on the packaging.
Of the countries that enacted MHM education policies in the A3 Policy Checklist, we found none that mention within their policy documentation the distribution of menstrual cups or other reusable products. Where there is mention of menstrual products, language and programming typically focuses on distribution of disposable products. As countries continue to draft policies that provide menstrual products, it is critical to urge an enabling environment for eco-friendly products where possible—not only in LMICs but in HICs, where menstruators can generally exercise greater choice and accessibility. For example, an evaluation report was released in 2018 detailing a pilot program in Scotland that delivered menstruators’ products of their choice, for free. Menstrual cups made up only 2% and reusable towels only 3% of the products distributed; in contrast, disposable sanitary towels (pads) made up 54%, tampons 15%, and a combination of the towels and tampons made up 19%. Interviews with menstruators revealed that many did not know that reusable materials existed, showing initial skepticism. Though many expressed interest in trying a reusable product, few participants followed through with using them.
Cup Concerns
Two major obstacles to menstrual cup uptake remain in LMIC contexts. A common hesitation for menstruators in LMICs entails concerns around inserting an object inside their bodies and reusing the cup. Menstrual hygiene management educational programs that have sought to promote cups often address these concerns and distribute kits including cups and other materials that help respond to these uncertainties as well as promote comfort with one’s body. For example, kits might include a small hand mirror for menstruators to not only help with inserting a menstrual cup, but to also enable an anatomy-based training that is sensitive to new users. Moreover, programs that promote peer and family support are underlined as critical to menstrual cup uptake. Targeting family support not only sensitively responds to sociocultural concerns around virginity and sexuality, but also the issue of privacy users express around routinely boiling or sterilizing their cups around other family members.
Emerging MHM Education
MHM education has yet to emerge as a standard in adolescent-focused policies, but in its early stages, offers opportunity for thoughtful design that integrates climate adaptation. As MHM policies gain uptake, HICs must also make greater efforts and contributions to minimizing climate change. Policymakers might include specific action items including:
✔ Requirements for programs that distribute menstrual products to offer sustainable options, i.e., menstrual cups or reusable pads
✔ Inclusion of menstrual product information within MHM education to inform menstruators about environmental impact of products as well as costs and benefits of products available on the market
✔ Increased partnerships or collaborations between development organizations/agencies and menstrual cup companies to commit to sustainable products
✔ Promote existing buy-one-give-one menstrual cup programs among HIC menstruators
✔ Invest in continued research on ecologically safe methods of menstrual product waste disposal and management
i We use the term “menstruators” here to include any person who menstruates, regardless of their gender identity.
This spring, the Population Council’s GIRL Center launched the Evidence for Gender and Education Resource (EGER), a searchable, easy-to-use, interactive database to drive better education results for girls, boys, and communities around the world. It includes information on current practice (who is doing what, where?), current evidence (what has worked in some settings?) and current needs (where do challenges remain?) in global girls’ education. Based on insights from EGER, we will be launching a 2021 Roadmap for Girls’ Education in the coming months.
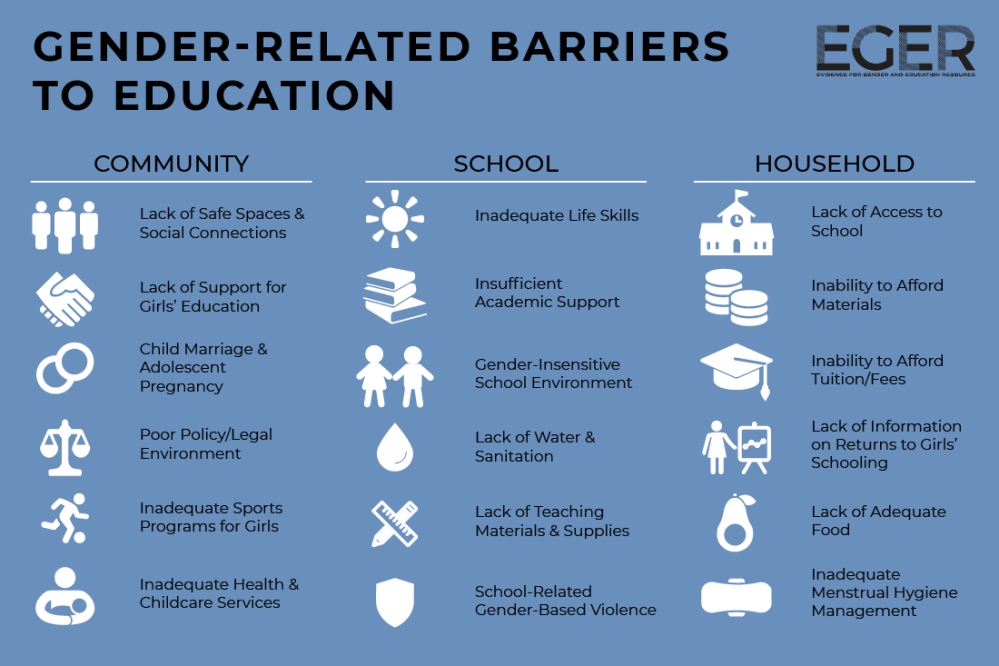
Before COVID-19 we were also seeing important—and persistent—gender-related barriers to school in many countries. To inform EGER, we conducted a systematic review of the evidence on what works to address gender-related barriers to schooling, and we developed a framework of perceived barriers. It shows gender-related barriers to education for girls at the community, school, and household levels. Underlying these barriers are two powerful forces: social norms and poverty.
Barriers at the school level are familiar—gender-insensitive school environments, lack of teaching materials and supplies, and school violence. But also important are barriers at the community and household levels, including child marriage, school access, and financial constraints.
Image credit: Evidence for Gender and Education Resource
While the full educational repercussions of COVID-19 have not yet unfolded, the pandemic is layering unprecedented pressures on top of existing challenges. But an important question for us to consider is this: In what ways have these barriers fundamentally changed due to COVID-19? And in what ways has COVID-19 simply exacerbated existing barriers?
WHAT, IF ANYTHING, HAS FUNDAMENTALLY CHANGED IN OUR WORK?
Since the beginning of the pandemic, the Population Council team in Kenya has partnered with the Executive Office of the President’s Policy and Strategy Unit to interview nearly 4,000 adolescent girls and boys by phone in four locations: Kisumu, Wajir, Kilifi, and the informal settlements in Nairobi.
For context—at least based on available data—after a peak in new cases in Kenya in November, new cases of COVID-19 are now declining, with about 200 per day at the end of December. So now the focus is on indirect effects of the pandemic—the effects of school closures, increasing economic strain, and challenges in accessing health care.
Connecting these two pieces of work—our current understanding of gender-related barriers to school, and a snapshot of what’s happening now in Kenya— how does COVID-19 change what we know?
1. Economic distress. Evidence from before COVID-19 tells us that addressing financial barriers to school can be effective not only to get young people into school, but potentially to close gender gaps, as well. Undoubtedly this remains true, even as the severity of economic barriers changes.
In Kenya, while most young people say they plan to go back to school upon reopening in January, we also see indicators of severe economic distress and a fear that inability to meet the costs of education will prevent reenrollment. For example, the majority of young people in three of the four settings in our study reported experiencing increased food insecurity due to COVID-19. This type of economic insecurity may well play out in terms of school access in the coming months and years.
2. Challenges in accessing education. We also know that expanding access to school—especially in settings where access is still a challenge—can be a very effective way to increase enrollment and close gender gaps. For example, school construction programs in countries like Burkina Faso or buying bicycles for girls in India, have been effective. But what does “access” mean now? How has that changed?
In Kenya, the majority of adolescents say they are doing some kind of schoolwork or learning at home during the pandemic, with the exception of Wajir, where fewer than 20 percent of 10- to 14-year-old girls, compared to 30 percent of 10- to 14-year-old boys indicated this was the case. When asked why they were not doing schoolwork at home, the most common reasons were that the school hasn’t provided lessons, and/or they needed to help with chores at home.
3. Importance of pedagogy. We have also seen over and over again that improving pedagogy, such as helping teachers adapt the curriculum to students’ different learning levels, is effective. What does this look like during and post-COVID-19? What models can we build on? (Hint: There are promising models out there already!)
In places like Wajir, where many young people have spent nearly a year without doing schoolwork or reading at home, ensuring school access is only the first step. Teachers will be faced with new challenges in helping students catch up and get back on track, with perhaps a broader range of skills in their classrooms than ever before.
Although it has been 10 months since the COVID-19 pandemic began, we’re only starting to see its effects—both direct and indirect—on school-age children and their families. As we think about what comes next, let’s not forget the fundamentals—what we already know about gender-related barriers to schooling, and what has worked to improve education for girls before. What we need to understand is how COVID-19 changes those fundamentals, and how we must change our plans in response.
This blog was first published on the Education Plus Development Blog on the Brookings Institution website.